Cardiovascular events may lead to medical incapacitation. Thus an estimation of the probability of an applicant suffering a cardiovascular (CV) event is an essential part of the assessment. Such estimation is based on community prevalence of ischaemia.
The General Direction, Timetable for Routine Examinations, prescribes when a formal cardiovascular risk assessment is required to be performed.
GD: Timetable for Routine Examinations [PDF 500 KB]
The General Direction, Examinations Procedures, prescribes how a formal cardiovascular risk assessment should be performed.
The General Direction, Examination Procedures, requires that a 5-year CV risk estimate of 10% or above requires exclusion of cardiac ischaemia.
GD: Examination Procedures [PDF 1.6 MB]
The information sheet, Cardiovascular risk, provides explanations for applicants. MEs may find the information useful.
Medical information sheet 007: Cardiovascular risk [PDF 626 KB]
Note: An applicant with a history of peripheral vascular disease, cerebrovascular accident or cardiovascular disease automatically falls in a high 5-year cardiovascular risk category, i.e. well above 10%.
In general a symptom limited, unequivocally negative, stress ECG reaching a good level of exercise (end of stage 3, i.e. 9 minutes or above of the Bruce protocol, 85% of maximum predicted, 10 METS) is acceptable evidence of absence of ischaemia.
When a stress ECG cannot be accomplished by exercise, a pharmacological stress test may be acceptable. The reason for undertaking such test must be explained and considered.
When required, the CAA acknowledged validity of such test is:
Part 5 of this manual provides CAA protocols for the various tests and their reporting.
The relevant protocol should be printed and given to the applicant to pass on to the practitioner conducting the test. This is to ensure a high quality stress is performed, that is useful for aviation public safety purposes.
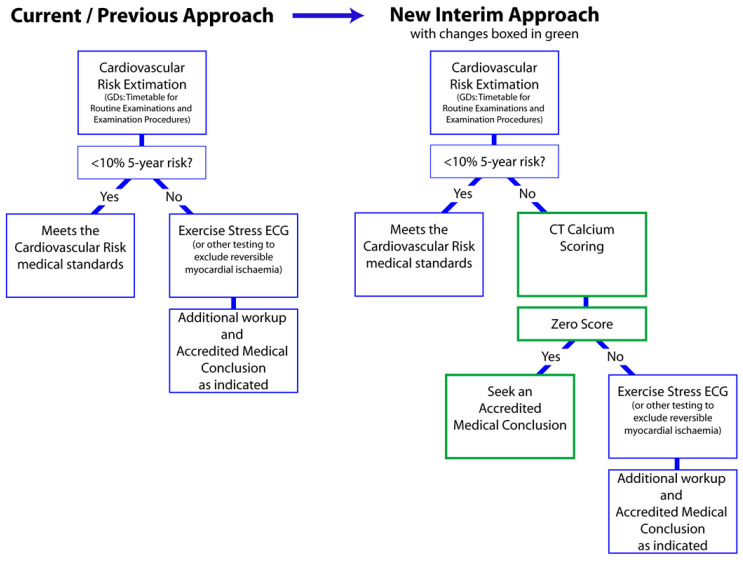
CT Coronary Artery Calcium Scoring (CT Calcium Scoring) is a relatively inexpensive test. Published research confirms the powerful prognostic value of a zero Agatston score.
For the purpose of the cardiovascular risk assessment, a Calcium Score of zero will allow to reassess the cardiovascular risk as being lower than suggested by the method prescribed in the GD 'Examination procedures'. A Calcium score of zero can be relied upon for several years.
Currently, until changes are made to several documents, this policy can only be implemented via the statutory process provided by sections 27B(2) and (3) of the Civil Aviation Act flexibility (Accredited Medical Conclusion).
At this point of time CAA will accept an Agatston score of zero as remaining valid for a period of five years.
So, currently:
This process is also shown here in diagram form.
In some cases a stress ECG is not sufficient to exclude ischaemia because of an insufficient level of exercise, a non-unequivocally negative or a positive tracing.
A stress echocardiogram or myocardial perfusion scan can be undertaken to more reliably exclude ischaemia. Other reasons to undertake such investigations may be the applicant’s cardiovascular history or a previous equivocal stress ECG. In doubt MEs should contact the CAA.
The role of other investigative modalities has not been clearly established in the context of aeromedical certification. MEs should consult with CAA whenever an applicant presents to them having undergone any other such investigations, including coronary angiography or CT coronary angiography.
See comments about CT Calcium Scoring that may affect the following list.